by Dr. A.N Rai | Jan 15, 2020 | Resources
What is the best perfume out and about for adult males there? We have no issue with Woman Supremacy as individual method of living, It’s my method of http://conwypirates.co.uk/portfolio/gallery7/ existence since my first 30 days of highschool. And being a natural aficionado is a whole lot unique than simply just experiencing one from period to period. (more…)
by Dr. A.N Rai | Jan 10, 2020 | Resources
Asia has a good simple medicine and health one that is administered at the talk about levels relatively than the national levels mostly. Beyond this one benefit, the programs vary on what they deal with with some programs getting even more in depth than other people. Tons of simple and easy making cookies recommendations with a better twist that flavour superb even so. (more…)
by Dr. A.N Rai | Jan 4, 2020 | Resources
An write-up analysis examines all the distinct elements of an write-up with the purpose of determining the complete idea of the write-up. Affirmative, one particular will definitely learn a new great deal of language from looking at and likewise have a new great deal of ideas into how different folks are convinced. Though at current, net advertising has been dominating over newspapers but the audience of newspapers has in no way declined. (more…)
by Dr. A.N Rai | Jan 3, 2020 | Resources
Connect 4 is normally a strategy video game played the two by simply youngsters and men and women tracing rear to 1974. Is packed whole of popularfree online video games. (more…)

by Dr. A.N Rai | Oct 16, 2019 | Resources
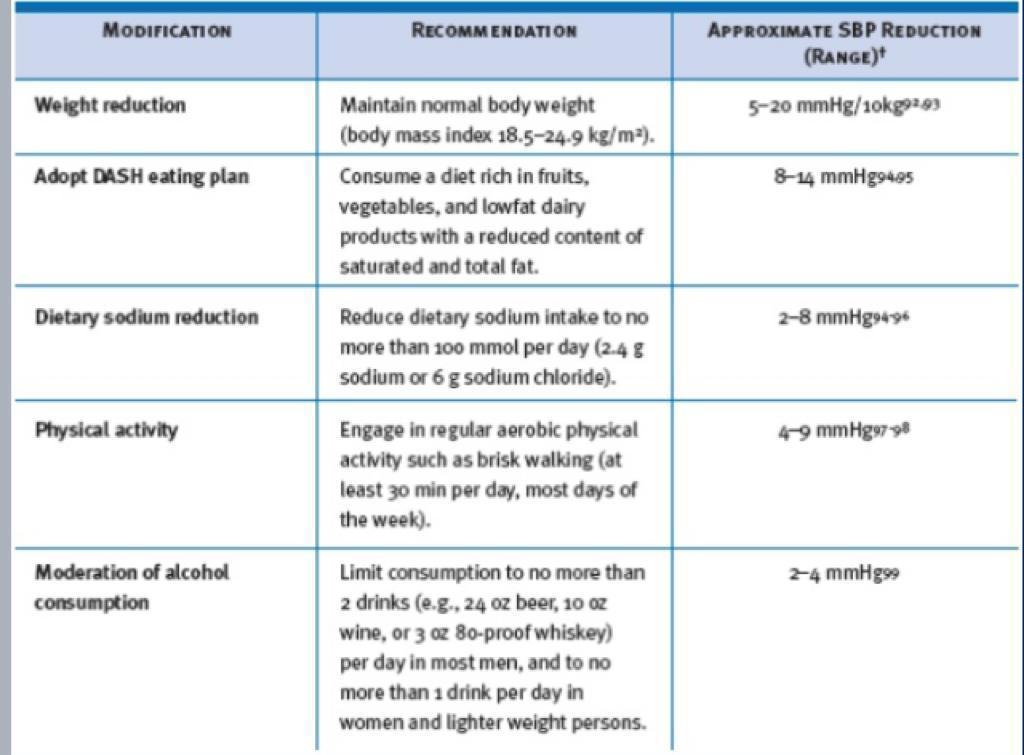
Several lifestyle interventions have been showed to reduce blood pressure. Apart from contributing to the treatment of hypertension, these strategies are beneficial in managing most of the other cardiovascular risk factors
In general, lifestyle changes should be regarded as a complement to drug therapy rather than an alternative.
by Dr. A.N Rai | Jun 20, 2019 | Resources
The blinking lighting and exciting jingles in casinos may encourage risky decision-making and potentially promote problem gambling behaviour, implies new research from the University of Uk Columbia. (more…)

